Dictation-based charting has various benefits in healthcare documentation, such as reduced cost and accurate documentation. When a provider dictates the content for charting, our advanced speech-to-text software accurately converts the recorded audio into text in a provider-specified format and style within minutes. This simplified documentation process of medical scribing services enables healthcare providers to cut down the cost of charting, document the exact information they require, and prevent unintentional disclosure of any confidential information with a third person. By facilitating higher documentation speed and accuracy, dictation-based charting increases the quality of patient care and workflow efficiency.
Dictation Based Charting Key Features
Provider-Directed Documentation
Healthcare providers directly dictate the content to be included in the documentation, providing specific instructions to the scribe. This allows for customization based on the provider’s preferences and ensures that the documentation accurately reflects the encounter.
Quality Assurance
Dictation-based charting undergoes stringent quality assurance measures such as proofreading, editing, and formatting to ensure the accuracy and completeness of the transcribed information. This helps maintain the integrity of the medical records and reduces the risk of errors.
Advantages of Dictation Based Charting
Accuracy
Dictation-based charting helps minimize errors often associated with manual typing, as documentation specialists can focus solely on listening and accurately transcribing the spoken words. This reduces the likelihood of documentation errors and ensures that medical documents are accurately maintained.
Customized Instructions
Healthcare providers provide specific instructions to the documentation specialists regarding the content and format. This customization allows personalized charting that aligns with the unique preferences and requirements of each provider.
Efficiency
Dictation-based charting significantly accelerates the documentation process. Providers can dictate patient notes in real-time or after the visit, reducing the time needed to complete medical records and freeing up more time for direct patient care.
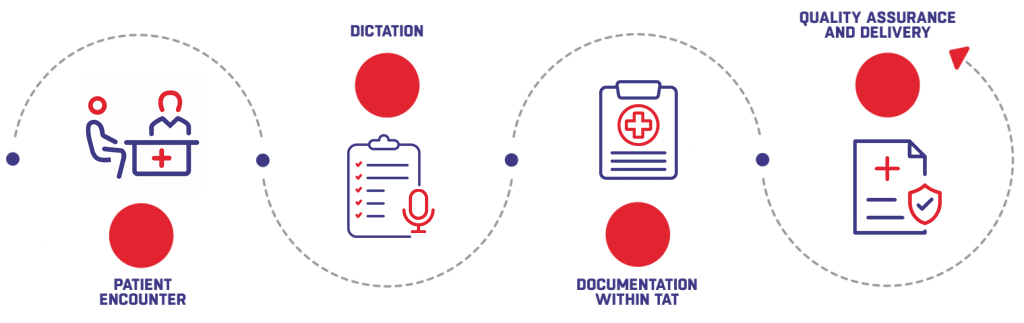
During the patient encounter or after the visit, the healthcare provider uses speech-to-text software to dictate relevant information to the documentation specialist, including the patient’s chief complaints, medical history, examination findings, diagnosis, and treatment plans.
Once the dictation is complete, the recorded audio files are transcribed into text format by a documentation specialist. Editing and formatting are completed within the specified turnaround time (TAT) to ensure the timely availability of patient records for subsequent care and decision-making.
Quality assurance processes involve additional checks for accuracy, completeness, adherence to documentation standards, and compliance with regulatory requirements. After the speech-to-text software generates the draft report, it is reviewed by a documentation specialist to ensure all details are correct and up to standard.
Once the quality assurance review is complete, the finalized documentation is then securely uploaded to the patient’s Electronic Health Record (EHR), ensuring seamless integration and compliance with healthcare regulations.