In this synchronous offering of medical scribing services, a virtual medical scribe, supported by text-to-speech ambient AI, provides remote assistance to healthcare providers by documenting provider-patient encounters in real-time via a virtual communication platform. They observe and listen to patient encounters ensuring meticulous entry of all relevant patient data into the Electronic Health Record (EHR).
Real-Time Charting key Features
Remote Assistance
We empower healthcare providers with real-time support during patient encounters. Our remote assistance tools enhance efficiency, enabling providers to focus on patient care while we handle the documentation.
Instantaneous Data
Entry Into EHR
Our dedicated scribes expertly input vital information into Electronic Health Records (EHR) as they listen and observe the physician’s actions. This ensures that every detail is captured accurately and promptly, streamlining the documentation process.
In-Sync Observation
and Documentation
Experience the advantage of real-time documentation. Our scribes diligently track the physician’s actions, documenting patient data concurrently to create a coherent and comprehensive medical record. This seamless integration fosters better communication and improves patient outcomes.
Advantages of Real-Time Charting
Enhancing Patient Experience
We empower healthcare providers with real-time support during patient encounters. Our remote assistance tools enhance efficiency, enabling providers to focus on patient care while we handle the documentation.
Decreased Physician Fatigue
With our dedicated scribes handling documentation, physicians can devote more energy to patient care, reducing burnout and fostering a healthier work-life balance.
Accelerating Documentation
Real-time charting by professional scribes ensures rapid completion of medical records, allowing for quicker decision-making, improved care coordination, and more time for physicians to focus on what matters most.
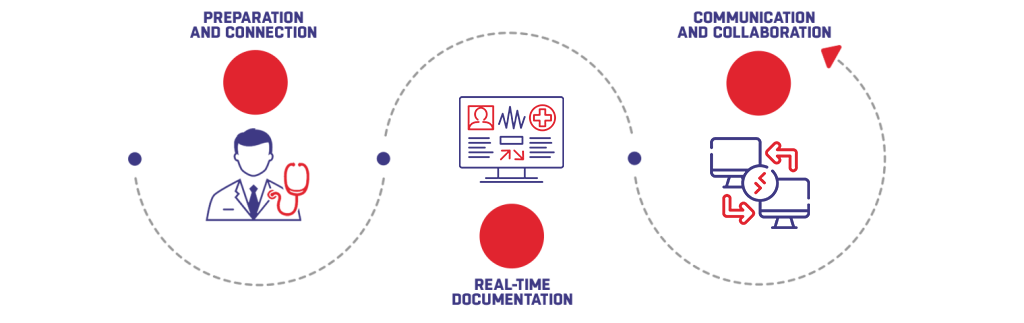
Our virtual scribes start by seamlessly connecting with your practice through Microsoft Teams. Once connected, they join the virtual meeting to observe the physician’s activities in real-time, ensuring a smooth and direct connection to your practice.
With precision and efficiency, our virtual scribes document every detail of the patient’s encounter directly into the Electronic Health Record (EHR). From medical history and diagnoses to treatment plans and prescriptions, our scribes ensure comprehensive and accurate records allowing physicians to focus entirely on patient care.
Maintaining clear and interactive communication throughout, our scribes are available via video or audio for real-time clarification. This ensures nothing is lost in translation and all patient information is accurately captured. Moreover, for seamless virtual interaction, Microsoft Teams is leveraged by strictly adhering to HIPAA regulations and data security measures to safeguard patient confidentiality.